Cognitive Distortions: How Unhelpful Thinking Affects Sleep, Anxiety, PTSD, and Recovery
By Dr. Charles R. Freeman, Ph.D.
Yes, the way you think can make sleep, anxiety, PTSD symptoms, and emotional distress worse. That does not mean your symptoms are your fault. It means that thoughts, emotions, physical symptoms, and behavior influence one another. When the mind gets stuck in fear-based or extreme thinking, the body often follows with tension, alertness, worry, and poor sleep.
Cognitive distortions are unhelpful thinking patterns that make a situation seem more hopeless, dangerous, permanent, or personal than it really is. These patterns are common during stress, trauma, chronic insomnia, depression, and anxiety. The mind takes shortcuts, especially when the nervous system is tired or on high alert.
The cognitive distortion framework was popularized by psychiatrist David Burns, M.D., in his influential book Feeling Good: The New Mood Therapy. I use these well-known cognitive behavioral therapy concepts in practical ways with patients dealing with sleep, anxiety, trauma, and recovery. The purpose is not to blame people for their symptoms. The purpose is to help patients recognize when the mind is turning fear, exhaustion, or past trauma into conclusions that may not be accurate.
What Are Cognitive Distortions?
Cognitive distortions are not character flaws. They are thinking habits. A person may automatically assume the worst, dismiss progress, blame themselves, or treat one setback as proof that nothing will ever improve. These thoughts can feel true in the moment, especially when the body is anxious, exhausted, or trauma-activated.
One of the most important recovery skills I teach is learning that thoughts are not always facts. A thought may be loud, familiar, and emotionally convincing, but that does not make it accurate. Cognitive behavioral therapy helps patients slow down, identify the thought, examine the evidence, and consider a more balanced response.
This is not the same as pretending everything is fine. Positive thinking does not solve insomnia, PTSD, or anxiety. The goal is accurate thinking, not forced optimism.
A Few Common Cognitive Distortions
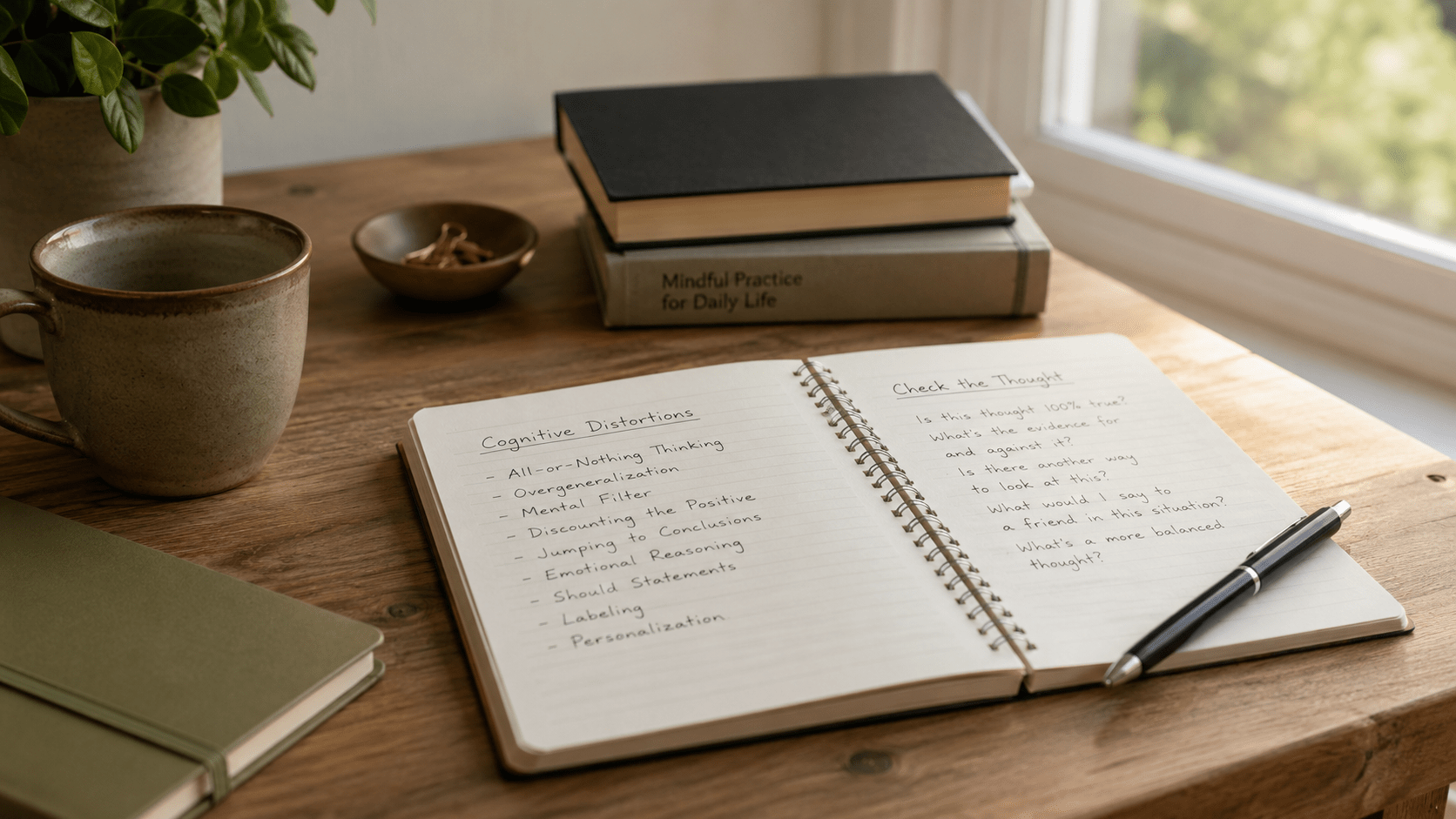
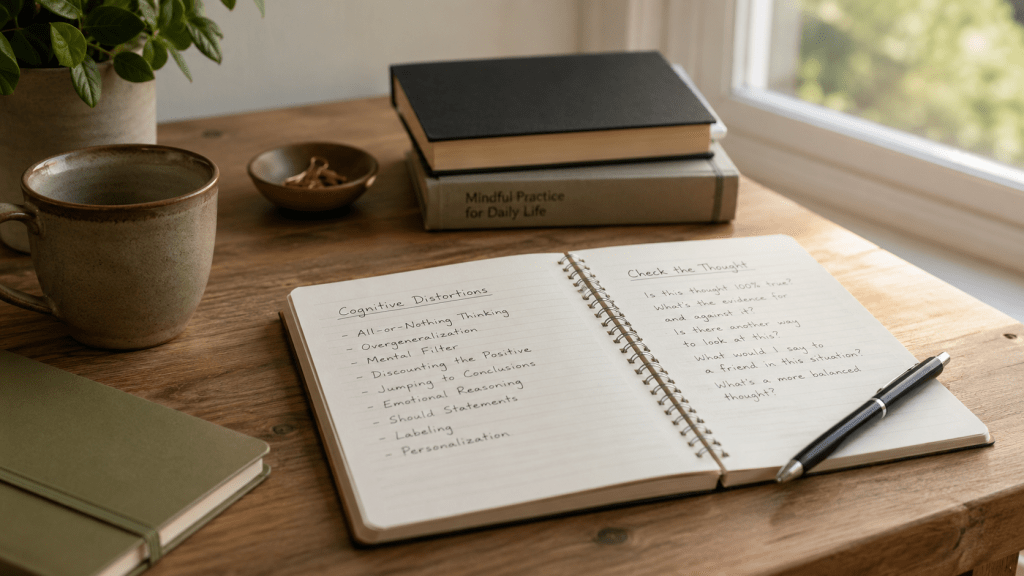
Some of the most common negative thinking patterns include all-or-nothing thinking, overgeneralization, mental filter, disqualifying the positive, jumping to conclusions, mind reading, fortune telling, magnification, minimization, emotional reasoning, should statements, labeling, mislabeling, and personalization.
Catastrophizing means exaggerating how bad something will be. A person may think, “If I do not sleep tonight, tomorrow will be a disaster.” That thought increases anxiety, which then makes sleep harder.
All-or-nothing thinking means seeing things in black-and-white categories. A patient may say, “If I had one bad night, my treatment is failing.” In reality, recovery usually includes progress, setbacks, adjustments, and more progress.
Fortune telling means predicting a negative outcome as if it has already been decided. Someone may think, “I know I will be awake all night,” even though the night has barely started.
Emotional reasoning means assuming that because something feels true, it must be true. A trauma survivor may feel unsafe in a calm room and conclude, “I am in danger.” The feeling is real. The conclusion may not match the present situation.
Personalization means taking responsibility for events that are not fully your responsibility. After trauma, a person may think, “I should have stopped it,” or “It was my fault.” This can create shame, self-blame, and ongoing emotional pain.
Mental filtering means focusing only on the negative detail while missing the larger picture. A patient may sleep better four nights in a week but focus only on the one terrible night.
Disqualifying the positive means rejecting progress as if it does not count. A patient may say, “I slept six hours, but that was just luck.” This keeps the mind locked onto failure rather than learning from improvement.
How Cognitive Distortions Affect Sleep
Cognitive distortions can play a major role in chronic insomnia. Many people do not only struggle with wakefulness. They struggle with fear about wakefulness. This is where sleep anxiety begins.
A person may think, “If I do not sleep tonight, tomorrow will be a disaster.” That is catastrophizing. Another person may think, “I have had insomnia for years. I will never get better.” That is overgeneralization and fortune telling. Someone else may wake up at 2 a.m. and think, “I am probably going to be awake all night.” That thought can quickly activate the body.
Over time, the bed can become associated with effort, frustration, and alertness. I often describe this as conditioned arousal. The person is exhausted, but the mind has learned to treat bedtime as a problem-solving session or performance test. The harder they try to force sleep, the more awake they become.
This is why treating insomnia often requires more than sleep hygiene. A dark room and a comfortable mattress may help, but they are usually not enough when the mind is catastrophizing, predicting failure, and monitoring the clock. This topic connects closely with Anxiety and Insomnia, Why Worry Keeps People Awake, and CBT-I.
How Cognitive Distortions Affect PTSD and Trauma Recovery
Trauma can change the way people interpret safety and threat. After trauma, the nervous system may stay alert long after the danger has passed. This can make cognitive distortions feel especially convincing.
A trauma survivor may see danger everywhere, assume the worst will happen, or interpret uncertainty as threat. A delayed text message may feel like abandonment. A noise outside may feel like danger. A small mistake may feel like proof of failure. These reactions are not weakness. They are often the result of a nervous system that learned to survive by staying vigilant.
Self-blame is also common after trauma. Personalization and emotional reasoning can become painful patterns. A person may think, “I feel guilty, so I must have done something wrong.” That is emotional reasoning. Guilt can be a symptom of trauma, not proof of responsibility.
Recovery often involves learning to challenge automatic assumptions. That may include asking, “Is this danger happening now, or is my nervous system remembering danger from before?” This is a natural internal link opportunity to Why Trauma Can Affect Sleep for Years and Why the Nervous System Stays Alert After Trauma.
What I Often See in Practice
In clinical practice, I often see people become trapped in cycles of worry about sleep. One difficult night becomes “I am back to square one.” Waking at 3 a.m. becomes “The whole night is ruined.” A tired morning becomes “Nothing works for me.” These thoughts are understandable, but they increase pressure on the next night.
I also see trauma survivors who assume they should already be “over it.” That should statement creates shame. Trauma recovery does not follow a neat timeline. The nervous system heals through safety, skill-building, emotional processing, and repetition.
Many patients dismiss progress because they focus only on setbacks. They may be sleeping longer, using fewer medications, having fewer panic symptoms, or recovering faster after bad nights, but their mental filter only notices what still hurts. Patients often improve when they learn to identify these distorted thinking patterns and respond to them differently.
Can Cognitive Distortions Be Changed?
Yes, cognitive distortions can be changed with practice. The first step is awareness. You learn to catch the thought instead of automatically believing it. Then you ask whether the thought is accurate, useful, complete, or exaggerated.
A practical CBT approach may include asking: What is the evidence for this thought? What is the evidence against it? Am I predicting the future? Am I blaming myself for something outside my control? Is there another explanation? What would I say to someone I cared about if they were thinking this way?
Change is gradual. I am not asking patients to erase every negative thought. That is not realistic. The goal is to learn to respond differently when those thoughts appear. That skill can reduce anxiety, soften sleep anxiety, support PTSD recovery, and help the body move out of chronic alertness.
Key Takeaways
- Cognitive distortions are common unhelpful thinking patterns, especially during stress, insomnia, anxiety, and trauma recovery.
- Thoughts are not always facts, even when they feel convincing.
- Catastrophizing, fortune telling, emotional reasoning, and personalization can intensify sleep anxiety and PTSD symptoms.
- CBT helps people challenge automatic assumptions and consider more balanced explanations.
- Recognizing distorted thinking is a skill that can reduce suffering and support recovery.
Frequently Asked Questions
Can cognitive distortions make insomnia worse?
Yes. Thoughts such as “I will never sleep” or “Tomorrow will be a disaster” can increase anxiety and physical arousal, making sleep more difficult.
Are cognitive distortions my fault?
No. These patterns often develop during stress, trauma, anxiety, or depression. The goal is not blame. The goal is learning skills to respond differently.
What is catastrophizing?
Catastrophizing means assuming the worst possible outcome. In insomnia, it may sound like, “If I wake up tonight, tomorrow is ruined.”
Can PTSD make thoughts feel more threatening?
Yes. Trauma can train the nervous system to scan for danger. That can make uncertain or ordinary situations feel unsafe.
Does CBT help with cognitive distortions?
Yes. CBT helps people identify distorted thoughts, test assumptions, look for evidence, and build more accurate ways of responding.
Conclusion
Cognitive distortions can affect sleep, anxiety, PTSD, and recovery because the mind and body are connected. A frightening thought can create physical tension. Physical tension can make the thought feel more true. That cycle can keep people awake, anxious, guarded, and discouraged.
The hopeful part is that these patterns can change. You can learn to identify unhelpful thinking patterns, challenge automatic assumptions, and respond with more balance. Recovery does not require perfect thinking. It requires practice, patience, and the willingness to notice when the mind is turning fear into fact.
About the Author
 Dr. Charles R. Freeman, Ph.D., is a psychologist specializing in insomnia, sleep disorders, PTSD, anxiety, trauma, and Cognitive Behavioral Therapy for Insomnia (CBT-I). He has more than 25 years of experience helping individuals improve sleep, emotional well-being, and overall quality of life through evidence-based treatment approaches. If you would like to learn more about treatment options or schedule a consultation, please contact Dr. Freeman.
Dr. Charles R. Freeman, Ph.D., is a psychologist specializing in insomnia, sleep disorders, PTSD, anxiety, trauma, and Cognitive Behavioral Therapy for Insomnia (CBT-I). He has more than 25 years of experience helping individuals improve sleep, emotional well-being, and overall quality of life through evidence-based treatment approaches. If you would like to learn more about treatment options or schedule a consultation, please contact Dr. Freeman.
The information in this article is provided for educational purposes only and is not intended to replace professional medical or psychological advice. Individual circumstances vary, and readers should consult a qualified healthcare professional regarding their specific concerns.