Can CBT-I Help You Sleep Without Medication?
By Dr. Charles R. Freeman, Ph.D.
Yes, Cognitive Behavioral Therapy for Insomnia, or CBT-I, can help many people sleep with less reliance on medication. CBT-I teaches the brain and body how to return to natural sleep by changing the thoughts, behaviors, habits, and nervous-system patterns that keep insomnia going. Medication may help temporarily, but CBT-I addresses the causes of chronic insomnia rather than only sedating the symptom.
That distinction is important. I do not tell patients to suddenly stop medication. Sleep medications, benzodiazepines, antidepressants, and other prescriptions should only be changed in coordination with the prescribing physician. My role is to help patients build skills so sleep does not depend entirely on an external substance.
Many people start taking something for sleep during a difficult season: grief, trauma, anxiety, medical stress, work pressure, divorce, caregiving, or a period of major life disruption. At first, the medication may help. Over time, some patients begin needing more support from pills, supplements, alcohol, or strict rituals. They may sleep, but the sleep does not feel restorative. They may also start believing, “I cannot sleep on my own anymore.”
What Is CBT-I?
CBT-I is a structured treatment for chronic insomnia. It is not simply sleep hygiene, relaxation, or positive thinking. It is a practical method for retraining the sleep system. CBT-I looks at what the person does before bed, how much time they spend awake in bed, how they respond to nighttime awakenings, what they believe about sleep, and how much fear has become attached to not sleeping.
In chronic insomnia, the bed often becomes associated with effort, frustration, clock watching, and fear. A person may feel sleepy in the living room, then become wide awake the moment they get into bed. That does not mean they are broken. It means the nervous system has learned a pattern. CBT-I helps change that pattern.
Why Medication Alone Often Does Not Solve Chronic Insomnia
Medication can sometimes provide short-term relief. The problem is that chronic insomnia is often the symptom, not the root cause. Underneath the sleep problem may be anxiety, trauma, PTSD, pain, depression, grief, over-responsibility, perfectionism, or a learned fear of being awake.
Sedation and healthy sleep are not the same thing. Restorative sleep supports memory, mood, emotional processing, immune function, concentration, and physical recovery. Some patients describe medication-induced sleep as “fake sleep.” They were unconscious, but they wake up foggy, unrefreshed, anxious, or still afraid of the next night.
CBT-I works differently. Instead of trying to knock the body out, it helps reduce the arousal that keeps the brain awake. It also helps patients rebuild confidence that their body can sleep naturally again.
What Is CBT-I Not?
CBT-I is not a list of generic tips. Many patients already know to keep the room dark, avoid caffeine late in the day, reduce screens, and maintain a consistent schedule. Those habits can help, but they are usually not enough when insomnia has become chronic.
CBT-I is also not willpower. Patients with insomnia are often trying very hard already. In fact, trying harder can make sleep worse. Sleep does not respond well to pressure. The more a person tries to force sleep, the more the brain treats bedtime as a performance test.
CBT-I is not about blaming the patient either. It is about identifying the patterns that are keeping the nervous system activated and then changing them in a careful, practical way.
How Does CBT-I Help You Sleep Without Medication?
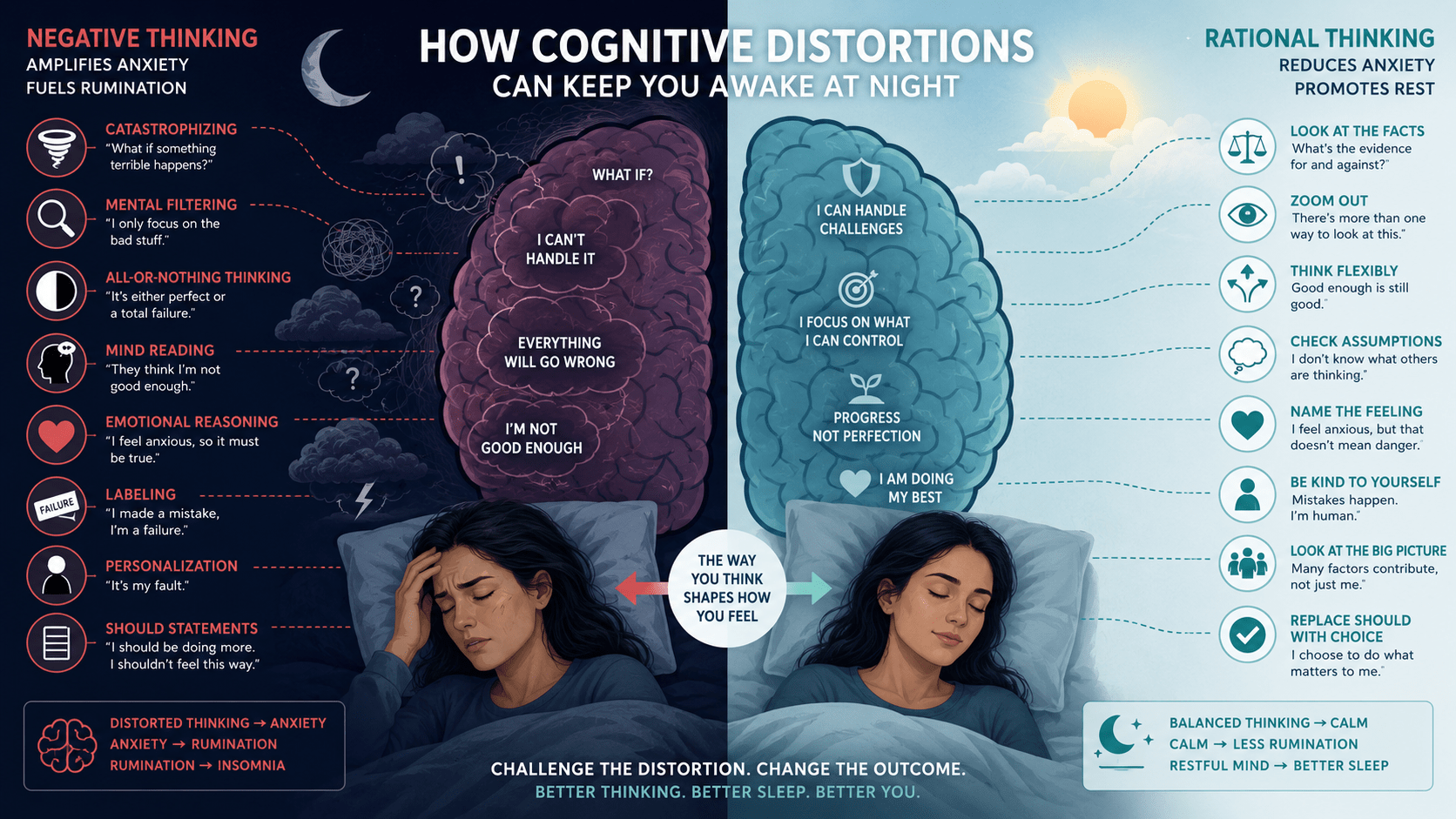
CBT-I helps by addressing conditioned arousal. Conditioned arousal means the brain has learned to connect bed, bedtime, or nighttime waking with alertness. The person may begin monitoring sleep, checking the clock, predicting failure, and worrying about the next day. A normal awakening becomes an emergency.
CBT-I teaches a different response. The patient learns how to reduce clock watching, decrease catastrophic thoughts, improve sleep timing, and stop reinforcing wakefulness in bed. Over time, the bed can become a cue for sleep again instead of a cue for effort.
One of the most important shifts is changing the relationship with wakefulness. Waking up during the night does not mean the night is ruined. A bad night does not mean the body has failed. When the patient stops reacting to wakefulness as a crisis, the nervous system often settles more quickly.
Can CBT-I Help If You Have Taken Sleep Medication for Years?
Many people can improve after years of relying on sleep aids, but the process needs to be handled responsibly. If medication has been used for a long time, especially benzodiazepines or sedative hypnotics, any change should be coordinated with the prescribing physician. Stopping suddenly can be unsafe.
The psychological work matters just as much. Long-term medication use can unintentionally teach the patient that natural sleep is impossible. CBT-I helps challenge that belief. The goal is not to rip away support before the person is ready. The goal is to build enough skill and confidence that sleep becomes less dependent on medication over time.
What Happens During CBT-I Treatment?
My approach is directive, collaborative, practical, and solution-focused. You are driving the car with your therapeutic goals, and I am the passenger helping guide the route. We look at what is maintaining the insomnia, create a treatment plan, assign practical homework, review what happened, fine-tune the tools, and continue adjusting until the changes become more sustainable.
Treatment may include sleep scheduling, stimulus control, cognitive restructuring, relaxation training, hypnosis, guided imagery, breathing skills, and strategies for reducing sleep anxiety. If trauma, PTSD, nightmares, or hypervigilance are involved, treatment may also include EMDR or other trauma-focused work. If pain or medical symptoms are involved, we may coordinate with physicians or other specialists.
CBT-I is not passive. The patient has to practice. The more energy the patient puts into the process, the more they usually get out of it. The goal is to leave the patient with tools they can use for the rest of their life.
What I Often See in Practice
I often meet patients who are capable, responsible, and exhausted. They may still work, parent, lead, care for others, and handle complex responsibilities. From the outside, they look functional. Inside, they are afraid of the next bad night.
Functioning is not the same as wellness. Many patients are getting through the day with adrenaline, caffeine, rigid routines, and fear. They do not need shame. They need a clear plan, clinical support, and repeated practice with skills that calm the nervous system.
Recovery does not always mean perfect sleep every night. It often means fewer catastrophic reactions, faster return to baseline, less fear of wakefulness, and more confidence in the body’s ability to recover. When that happens, sleep becomes less fragile.
Key Takeaways
- CBT-I can help many people sleep with less reliance on medication.
- Medication may provide short-term relief but may not address the root causes of insomnia.
- CBT-I is not just sleep hygiene, relaxation, or willpower.
- CBT-I targets sleep anxiety, conditioned arousal, clock watching, and fear of wakefulness.
- Medication changes should always be coordinated with the prescribing physician.
Frequently Asked Questions About CBT-I and Sleeping Without Medication
Can CBT-I replace sleeping pills?
For some people, CBT-I can reduce or eliminate reliance on sleeping pills over time. This should be done carefully and, when medication is involved, in coordination with the prescribing physician.
How long does CBT-I take to work?
Some people notice improvement within several weeks. Long-standing insomnia, trauma, anxiety, chronic pain, or medication dependence may require more time and a broader treatment plan.
Is CBT-I just sleep hygiene?
No. Sleep hygiene focuses on basic sleep habits. CBT-I is a structured treatment that addresses the thoughts, behaviors, conditioning, and physiological arousal that keep insomnia going.
Can CBT-I help if anxiety keeps me awake?
Yes. CBT-I helps reduce sleep anxiety, catastrophic thinking, clock watching, and fear of being awake. If anxiety is severe, anxiety treatment may also be part of the plan.
Can CBT-I help if trauma or PTSD affects my sleep?
Yes. When trauma is part of the insomnia cycle, CBT-I may be combined with EMDR, grounding, hypnosis, relaxation training, and other trauma-focused approaches.
Conclusion
CBT-I can help many people sleep without depending entirely on medication because it teaches the nervous system a different pattern. Instead of treating wakefulness as an emergency, patients learn how to reduce fear, retrain the bed as a cue for sleep, and address the root causes that keep insomnia active.
The goal is not simply to get through another night. The goal is restorative sleep, better emotional regulation, and practical skills that continue working long after treatment ends. When patients learn that their body can recover, sleep often becomes less of a battle and more of a natural biological process again.
About the Author
 Dr. Charles R. Freeman, Ph.D., is a psychologist specializing in insomnia, sleep disorders, PTSD, anxiety, trauma, and Cognitive Behavioral Therapy for Insomnia (CBT-I). He has more than 25 years of experience helping individuals improve sleep, emotional well-being, and overall quality of life through evidence-based treatment approaches. If you would like to learn more about treatment options or schedule a consultation, please contact Dr. Freeman.
Dr. Charles R. Freeman, Ph.D., is a psychologist specializing in insomnia, sleep disorders, PTSD, anxiety, trauma, and Cognitive Behavioral Therapy for Insomnia (CBT-I). He has more than 25 years of experience helping individuals improve sleep, emotional well-being, and overall quality of life through evidence-based treatment approaches. If you would like to learn more about treatment options or schedule a consultation, please contact Dr. Freeman.
The information in this article is provided for educational purposes only and is not intended to replace professional medical or psychological advice. Individual circumstances vary, and readers should consult a qualified healthcare professional regarding their specific concerns.