
Sleep Anxiety and Insomnia: Why Fear of Not Sleeping Keeps You Awake
By Dr. Charles R. Freeman, Ph.D.
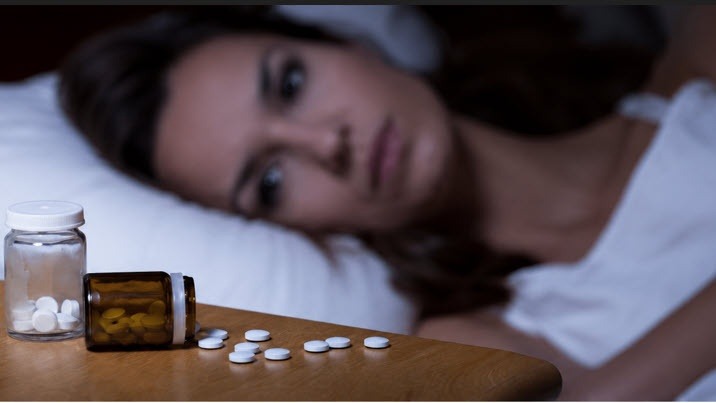
Sleep anxiety can keep insomnia going because the fear of not sleeping activates the same nervous system response that prevents sleep. The person may be exhausted, but the mind starts monitoring, calculating, predicting failure, and worrying about tomorrow. At that point, the first treatment target is often not sleep itself, but fear of not sleeping.
This is a very common pattern. A person has a few bad nights. Then they start watching the clock. They worry about work, parenting, driving, health, mood, or whether insomnia is “coming back.” Bedtime stops feeling like rest and starts feeling like a test. Sleep is not a performance. It is a biological process that improves when the patient stops turning it into a test.
Many patients do not need more sleep rules. They need less fear around sleep. Sleep hygiene can be useful, but chronic insomnia usually needs more than a colder bedroom, a darker room, or a new supplement. Good treatment looks at the loop, not only the loudest symptom.
What Is Sleep Anxiety?
Sleep anxiety is fear about falling asleep, staying asleep, waking too early, or being unable to function the next day. It may show up as racing thoughts, body tension, panic, clock checking, frustration, or a sense of dread as bedtime approaches.
Many insomnia patients do not fear being awake itself. They fear what wakefulness means. They may think, “I will not be able to work tomorrow,” “My health is being damaged,” “I am losing control,” or “Something is wrong with me.” The body hears those thoughts as danger. The heart rate may rise. Muscles tighten. Breathing changes. The nervous system moves toward fight-or-flight when the person needs the opposite.
For many patients, wakefulness is not the enemy. Panic about wakefulness is the enemy. Once the brain learns that being awake at night is dangerous, it becomes more alert at the exact time the person wants to rest.
Why Does Trying Harder to Sleep Make Insomnia Worse?
Trying harder often makes insomnia worse because sleep does not respond well to pressure. The harder patients try to sleep, the more they teach the brain that bedtime is a performance test. That effort can look responsible from the outside, but it feels exhausting from the inside.
High achievers are especially vulnerable to this pattern. The same control style that helps a person perform during the day can keep the nervous system activated at night. They analyze the night. They compare it to previous nights. They adjust the routine again and again. They use discipline, supplements, medication, rigid rules, or sleep tracking to regain control.
The problem is that the bed becomes a place to plan, judge, rehearse, monitor, and argue with yourself. Over time, the nervous system learns bedtime the same way it learns danger: through repetition, association, and emotion.
How Does One Bad Night Turn Into Chronic Insomnia?
A bad night becomes chronic insomnia when the patient starts organizing life around preventing the next bad night. This may include spending too much time in bed, canceling activities, avoiding travel, tracking sleep obsessively, taking something every night “just in case,” or treating every awakening as an emergency.
One poor night of sleep is uncomfortable. It may affect mood, energy, concentration, and patience. But one bad night is not a relapse. The patient’s reaction to the bad night determines whether the insomnia loop grows stronger or weaker.
When someone wakes up at 2 or 3 a.m. and thinks, “Here we go again,” the nervous system may escalate. The person checks the clock, calculates remaining sleep, predicts failure, and becomes more awake. The effort to return to sleep becomes more disruptive than the awakening itself.
Is Insomnia Sometimes the Symptom Rather Than the Root Cause?
Yes. Insomnia is often the symptom, not the root cause. Chronic insomnia rarely appears as a stand-alone sleep problem. It often sits inside a larger system involving anxiety, trauma, pain, medical symptoms, family pressure, perfectionism, relationship stress, occupational strain, or loss of control.
Sleep disturbance acts as a symptom amplifier. Poor sleep worsens irritability, anxiety, pain tolerance, mood stability, concentration, decision-making, and relationship strain. Then those problems feed back into worse sleep. That is why effective treatment does not simply ask, “How do we knock you out?” It asks, “What is keeping your nervous system from standing down?”
Trauma can also be a major contributor. Trauma does not always announce itself as a flashback. It may appear as early waking, nightmares, body tension, anger, shame, emotional withdrawal, or an inability to relax. The body may be safe now, but the nervous system may still be operating under old orders.
How Does CBT-I Help Sleep Anxiety?
Cognitive Behavioral Therapy for Insomnia, or CBT-I, is the gold standard treatment for chronic insomnia. CBT-I is not simply sleep hygiene. It is a structured treatment that addresses the thoughts, behaviors, and nervous-system patterns that keep insomnia alive.
CBT-I helps patients understand why insomnia continues. It may include sleep scheduling, stimulus control, reducing clock watching, changing catastrophic sleep thoughts, and learning how to respond to wakefulness without making it stronger. The clinical target is often the patient’s response to wakefulness. When patients stop escalating after an awakening, sleep often becomes less fragile.
Acceptance-based strategies can also strengthen CBT-I. Patients benefit when they practice tolerating uncertainty, letting go of struggle, and allowing wakefulness without turning it into a crisis. This does not mean giving up. It means no longer feeding the nervous system the message that wakefulness is dangerous.
What I Often See in Practice
I often see patients who are employed, respected, dependable, and outwardly successful while privately living with serious sleep anxiety. Functioning is not the same as being well. Many people remain productive through suppression, adrenaline, rigid routines, fear, and endurance. That does not mean they are not impaired.
I also see patients who have lost confidence in their body’s ability to sleep naturally. They may depend on medications, alcohol, supplements, or highly rigid rituals because they fear being awake and doubt their ability to recover. Sleep medication concerns often reflect a deeper fear: “What if my body cannot do this on its own?” Medication decisions should always be discussed with the prescribing physician, but long-term improvement usually requires more than symptom suppression.
The first sign of recovery may not be a perfect night. It may be a calmer response to the same old symptom. A patient wakes up, notices anxiety, and does not panic. They have a bad night and do not organize the next day around fear. Recovery is often measured by the speed of return to baseline.
What Helps Break the Sleep Anxiety Cycle?
Breaking the sleep anxiety cycle usually requires a practical approach that teaches patients specific skills. Patients learn how insomnia works, how the nervous system learns fear, and how their own nighttime responses can keep the pattern going. Treatment may include CBT-I for chronic insomnia and conditioned arousal, reduced clock watching and sleep tracking, and new ways to respond to awakenings without panic. Stimulus control can help the brain reconnect the bed with sleep instead of struggle. EMDR or trauma-focused treatment may help when trauma plays a role. Hypnosis, guided imagery, breathing, and grounding skills can also support the process. Exercise, nutrition, sound sleep habits, and meaning or spiritual connection may strengthen recovery. As sleep improves, patients often feel more emotionally steady, more physically resilient, and more confident in daily life.
Key Takeaways
- Sleep anxiety keeps insomnia going by making wakefulness feel dangerous.
- The harder patients try to force sleep, the more bedtime can become a performance test.
- One bad night is not a relapse. The reaction to the bad night matters.
- Insomnia is often connected to anxiety, trauma, pain, perfectionism, over-responsibility, or conditioned arousal.
- CBT-I helps patients change the thoughts, behaviors, and nervous-system patterns that maintain chronic insomnia.
Frequently Asked Questions
What is sleep anxiety?
Sleep anxiety is fear about falling asleep, staying asleep, waking too early, or not functioning the next day. It often involves clock watching, catastrophic thinking, body tension, and panic about being awake.
Can worrying about sleep cause insomnia?
Yes. Worrying about sleep can train the nervous system to associate bedtime with pressure and danger. Over time, the bed may become connected with wakefulness instead of rest.
Why do I panic when I wake up at night?
You may panic because your brain interprets waking as a sign that the night is ruined. Treatment helps you respond to awakenings without clock checking, self-judgment, or catastrophic predictions about tomorrow.
Why does insomnia get worse when I try harder to sleep?
Trying harder can make sleep feel like a performance. Effort, analysis, and pressure increase arousal. Sleep usually improves when the nervous system stops receiving the message that wakefulness is an emergency.
Can CBT-I help sleep anxiety?
Yes. CBT-I helps reduce sleep-related fear, conditioned arousal, clock watching, and behaviors that keep insomnia going. It teaches patients how to respond to wakefulness in a way that weakens the insomnia loop.
Conclusion
Sleep anxiety is not a character flaw. It is a learned nervous-system pattern. The brain has learned that bedtime, wakefulness, or a bad night means danger. That pattern can be unlearned.
Many patients improve when they stop asking, “How do I make this symptom disappear?” and start asking, “How do I respond without making it stronger?” That shift is often the beginning of real recovery. The goal is not perfect sleep every night. The goal is greater confidence, less fear, and a stronger return to baseline when life or sleep becomes difficult.
About the Author
 Dr. Charles R. Freeman, Ph.D., is a psychologist specializing in insomnia, sleep disorders, PTSD, anxiety, trauma, and Cognitive Behavioral Therapy for Insomnia (CBT-I). He has more than 25 years of experience helping individuals improve sleep, emotional well-being, and overall quality of life through evidence-based treatment approaches. If you would like to learn more about treatment options or schedule a consultation, please contact Dr. Freeman.
Dr. Charles R. Freeman, Ph.D., is a psychologist specializing in insomnia, sleep disorders, PTSD, anxiety, trauma, and Cognitive Behavioral Therapy for Insomnia (CBT-I). He has more than 25 years of experience helping individuals improve sleep, emotional well-being, and overall quality of life through evidence-based treatment approaches. If you would like to learn more about treatment options or schedule a consultation, please contact Dr. Freeman.
The information in this article is provided for educational purposes only and is not intended to replace professional medical or psychological advice. Individual circumstances vary, and readers should consult a qualified healthcare professional regarding their specific concerns.